Emergency department corridor care and crowding is routine, UK wide & associated with patient harm.
This research describes in detail the scale of corridor care in UK Emergency Departments (EDs). It uncovers the associations between corridor care and ED occupancy and adverse patient outcomes such as length of stay and mortality.
About the research
Emergency Department crowding occurs when the number of patients requiring care within the ED exceeds the number of spaces designed for patient care. One consequence of crowding is the use of spaces not designed for patient care, collectively known as escalation areas. These spaces include hospital corridors and more recently the term ‘corridor care’ has been adopted by NHS England to cover all such care. NHS England aims to eliminate corridor care entirely and has published guidance stating that certain patient groups such as children and those presenting due to mental health issues should not be exposed to corridor care.
The UNCORKED study (Understanding Corridor and Escalation Area Care in UK Emergency Departments) was an observational study that involved 165 EDs across the whole of the UK, collecting data in March 2025. It aimed to establish what proportion of patients attending the ED experience corridor care, which patients are more likely to be affected and whether experiencing corridor care is associated with key outcomes such as hospital length of stay and 28 day mortality. The study also measured overall ED occupancy and the availability of resuscitation cubicles for patients requiring the most urgent care.
Policy implications
- NHS England and the devolved nation health systems should routinely and transparently report corridor care use and ED occupancy. The framework for doing this should be developed alongside clinical teams and facilitate capture of the broad variety or substandard care environments that are used.
- Length of hospital stay, increased ED occupancy and increased mortality should be considered key outcome-related ED performance metrics.
- Interventions to reduce ED corridor care should most urgently focus on those disproportionately affected: older patients and those from more deprived background across the UK and patients attending hospitals in Northern Ireland and Wales.
- Improving flow through the ED and into inpatient ward beds should be the primary focus of efforts to reduce ED corridor care and occupancy. This focus needs to be driven at a national policy level and involve system wide solutions.
Key findings
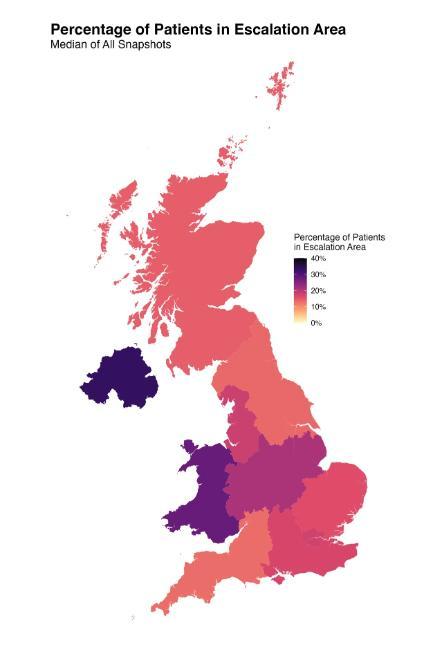
- 1 in 3 patients experienced corridor care at some point during their ED stay. Corridor care is the norm UK wide with regional variation. Corridor care was in almost all (95.7%) of the 165 participating EDs. The worst affected regions were Northern Ireland and Wales. Older patients and those from more socioeconomically disadvantaged areas were more likely to experience corridor care. Children and patients presenting with mental health issues were consistently seen to be exposed to corridor care throughout the study.
- Corridor care is associated with worse patient outcomes and significant opportunity cost. In those admitted to an inpatient bed, from the ED, being cared for in a corridor was associated with a 22% longer hospital stay. Every 10 patients experiencing corridor care is associated with 16 extra bed days (95% CIs 5 to 27 days). This equates to an annual opportunity cost of £389.1 million (95% CI £121.6 million - £656.7 million) on extra NHS bed days. Longer time spent in a corridor in the ED was associated with an increased risk of death at 28 day follow up.
- Higher mortality rates are observed in crowded (high occupancy) EDs. Being cared for in any area of an ED that was over 100% occupancy was associated with an increased risk of death at 28 days.
- Patients experience corridor care in the days before death. The majority of patients admitted to an inpatient bed from the ED who had died by 28 days, experienced corridor care in the ED, some on the same day that they died.
- Capacity to deal with critically ill patients is limited. At its worst, 1 in 4 EDs had no immediately available resuscitation area cubicle, impairing their ability to immediately deal with the sickest patients needing time critical care.
- Lack of flow into inpatient beds is the key issue. Throughout the study period the number of patients waiting in ED for a bed on an inpatient ward consistently exceeded the number of patients being cared for in corridors within the ED. If these patients had moved to inpatient beds, there would have been no corridor care in UK EDs. Average length of stay in EDs for those admitted to hospital was 16 hours.
Further information
Trainee Emergency Research Network (TERN) Understanding corridor and escalation area care in 165 UK emergency departments: a multicentre cross-sectional snapshot study Emergency Medicine Journal 2026; 43:72-80.
Main image generated using AI
The authors
Fraser Birse, North Bristol NHS Trust
Ben Clarke, Royal College of Emergency Medicine, NHS Lothian
Ryan McHenry, University of Glasgow, ScotSTAR and EMRS,
Dr Tom Roberts, Univeristy of Bristol on behalf of the Royal College of Emergency Medicine (RCEM) Trainee Emergency Research Network (TERN)