Michael A. Adams BSc, PhD
Research theme: 'The Biomechanics of Back Pain'
Back pain is a major problem for modern society, affecting most people at some time in their lives. People don’t die from it, but some can lose the enthusiasm for living and become chronically disabled, so the economic impact (in terms of work absenteeism) is great. We now know that most severe and chronic back pain emanates from the intervertebral discs, and most of the recent research has been directed towards understanding how and why these structures fail so often and so painfully in middle age. Genetic inheritance explains a great deal of the variance in “who gets” disc degeneration, but mechanical loading and other environmental factors are required to explain why the lower lumbar discs are affected so often, and why symptoms usually appear in early middle age, especially in those with physically-demanding jobs. In addition, the human personality plays a major role in all aspects of back pain “behaviour”, including pain perception, responses to treatment, and the decision to take time off work.
Accordingly back pain research is multi-disciplinary, with matrix biologists, geneticists, biochemists, psychologists and engineers all attempting to explain aspects of the phenomenon in their own terms. In a recent book ("The Biomechanics of Back Pain", by MA Adams, N Bogduk, K Burton, and P Dolan, Churchill Livingstone, Edinburgh, 3rd Edition 2012) we summarised our own approach to back pain research as follows:
‘The biomechanics of back pain’ does not imply a bias towards mechanical explanations of back pain; it merely reflects the fact that mechanical factors are the most obvious and preventable influences in a complex natural history which involves biological and psychological processes as well as mechanical ones (hence ‘bio-mechanics’). The title is also intended to imply a mechanistic approach to back pain, in which our knowledge of the biological and physical sciences is applied to explaining the various chains of events which lead to back pain. Back pain is certainly a difficult and multifaceted problem, but it is not so difficult that we must abandon the normal scientific method in favour of some vague holistic approach. Back pain should be explained, not explained away.
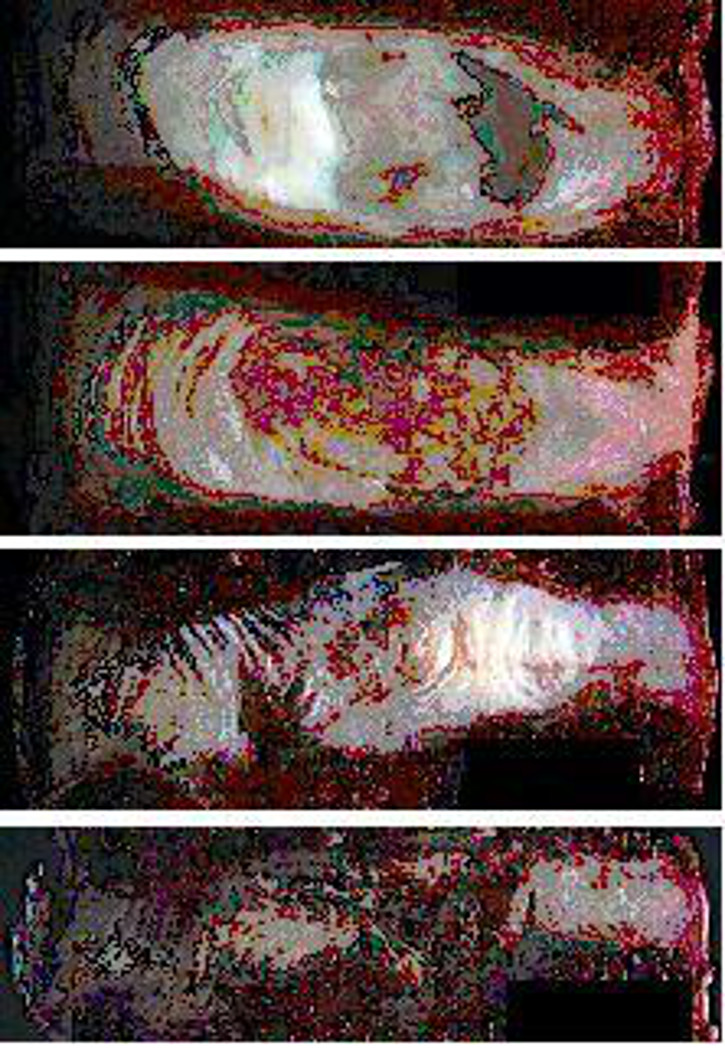
Figure 1 Human lumbar intervertebral discs sectioned in the mid-sagittal plane (anterior on the left). From top to bottom the images show: a healthy young adult disc; a healthy middle aged disc; a young degenerated disc; and a young severely degenerated disc.
Our recent research has attempted to explain how injury to an intervertebral disc can drive a degenerative process that is akin to ‘frustrated healing’. In cadaveric spines, we use a miniature pressure transducer to examine how injury to a disc (or to an adjacent vertebra) alters the mechanical environment of disc cells in ways that would affect their metabolism. We combine this technique with an optical strain measurement system to examine how disc degeneration can lead to other spinal problems including “segmental instability”, osteophytosis, apophyseal joint osteoarthritis, degenerative scoliosis, and senile kyphosis or “dowager’s hump”. Similar methods are used to investigate how injury to the cartilage of human synovial joints can lead to cartilage deterioration, and subsequently to osteoarthritis.
Our most recent concern is to explain why degenerated discs are so painful. There is increasing evidence that pain emanates from the disc periphery (outer anulus, and endplate) which is where the nerves are, and where injury most often occurs. Unfortunately, disc research is traditionally devoted to explaining age-related deterioration of the disc centre, even though this region of the disc is unlikely to painful, and is incapable of healing. A shift of focus is required: healing and pain relief should be the primary goals, not the reversal of ageing, which may well prove to be too difficult. Current research is exploring the physical consequences of disc disruption, by characterising the mechanical and biochemical micro-environment within anulus fissures. We suspect that focal reductions in pressure and proteoglycan concentration can alter cell-matrix binding, and initiate a series of pathological events including cell apoptosis, matrix degradation and re-innervation.
Chief collaborators in Bristol:
Trish Dolan and Mo Sharif (Anatomy), Kate Robson-Brown (Archaeology and Anthropology), John Tarlton (Clinical Veterinary Sciences) and Ian Harding (Medicine).
Selected recent publications
- Adams MA, Dolan P (2012). Intervertebral disc degeneration: evidence for two distinct phenotypes. Journal of Anatomy (accepted for publication).
- Stefanakis M, Al-Abbasi M, Harding I, Pollintine P, Dolan P, Tarlton J, Adams MA. (2012). Annulus fissures are mechanically and chemically conducive to the ingrowth of nerves and blood vessels. Spine (October 2012).
- Al-Rawahi M, Luo J, Pollintine P, Dolan P, Adams MA (2011). Mechanical function of vertebral body osteophytes, as revealed by experiments on cadaveric spines. Spine 36 10 770-7.
- Adams MA, Stefanakis M, Dolan P (2010). Healing of a painful intervertebral disc should not be equated with reversing disc degeneration. Clinical Biomechanics 25 961-71.
- Pollintine P, Luo J, Offa-Jones B, Dolan P, Adams MA (2009). Bone creep can cause progressive vertebral deformity. Bone 45(3) 466-72.
- Adams MA, Dolan P, McNally DS (2009). The internal mechanical functioning of intervertebral discs and articular cartilage, and its relevance to matrix biology. Matrix Biology 28: 384-89.
- Adams MA, Pollintine P, Tobias JH, Wakley GK, Dolan P (2006). Intervertebral disc degeneration can predispose to anterior vertebral fractures in the thoracolumbar spine. J Bone Miner Res 21:1409-16.
- Adams MA, Roughley PJ (2006). What is Intervertebral Disc Degeneration, and What Causes It? Spine 31:2151-61.
- Adams MA, Dolan P (2005). Spine biomechanics. J Biomech 38:1972-83.

Southwell Street, Bristol BS2 8EJ