Preventing the deaths of people experiencing homelessness
The number of people dying while experiencing homelessness is increasing every year. People who are homeless die younger and are more likely to die whatever their age, but there is widespread regional variation within England and across the whole UK.
Many of these deaths are preventable and the causes of death of people experiencing homelessness are very different to the rest of the population. Deaths of people in England and Wales who are homeless are much more likely to be referred to a Coroner for investigation.
Where a Coroner identifies that other lives can be saved, they must write to someone who can act to prevent other deaths. Examining these concerns from Coroners, this research identifies an exponential increase in reports from Coroners highlighting deaths connected to homelessness and precarious housing. Importantly, increasing numbers are sent specifically to organisations responsible for housing, including the Ministry of Housing, Communities and Local Government (MHCLG). From an average of one a year in 2017-21, a Coroner’s report is now sent to a housing authority every 8 weeks. Concerns in these reports about issues which could cause future deaths include:
- the impact of a lack of social housing;
- the bedroom tax;
- failures in providing adequate accommodation for people with intersecting vulnerabilities. This included those leaving care and young gay and trans people.
These reports demonstrate the ways in which the contemporary housing crisis causes death. This research highlights the need for urgent action to save lives, including improvements in the inquest process.
Regional Differences in England
1142 people experiencing homelessness died in England in 2024, a 14% increase on figures reported in 2023.
At a regional level, London has the highest number of deaths that we know of (326) while the North East had the fewest (46). When population is taken into consideration, the South West region has the second highest rate of reported deaths in England behind only London.
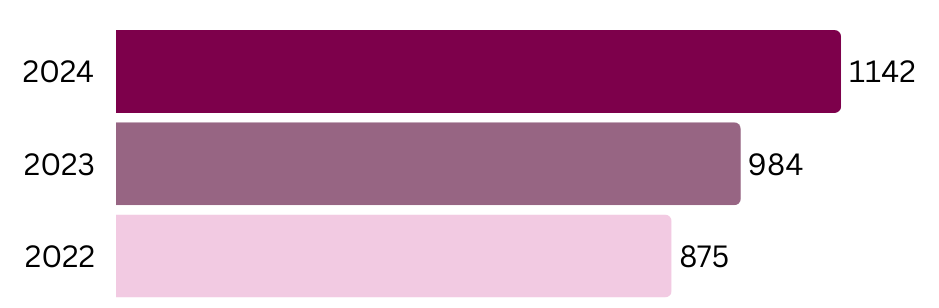
Number of reported deaths in England between 2022 and 2024 across England
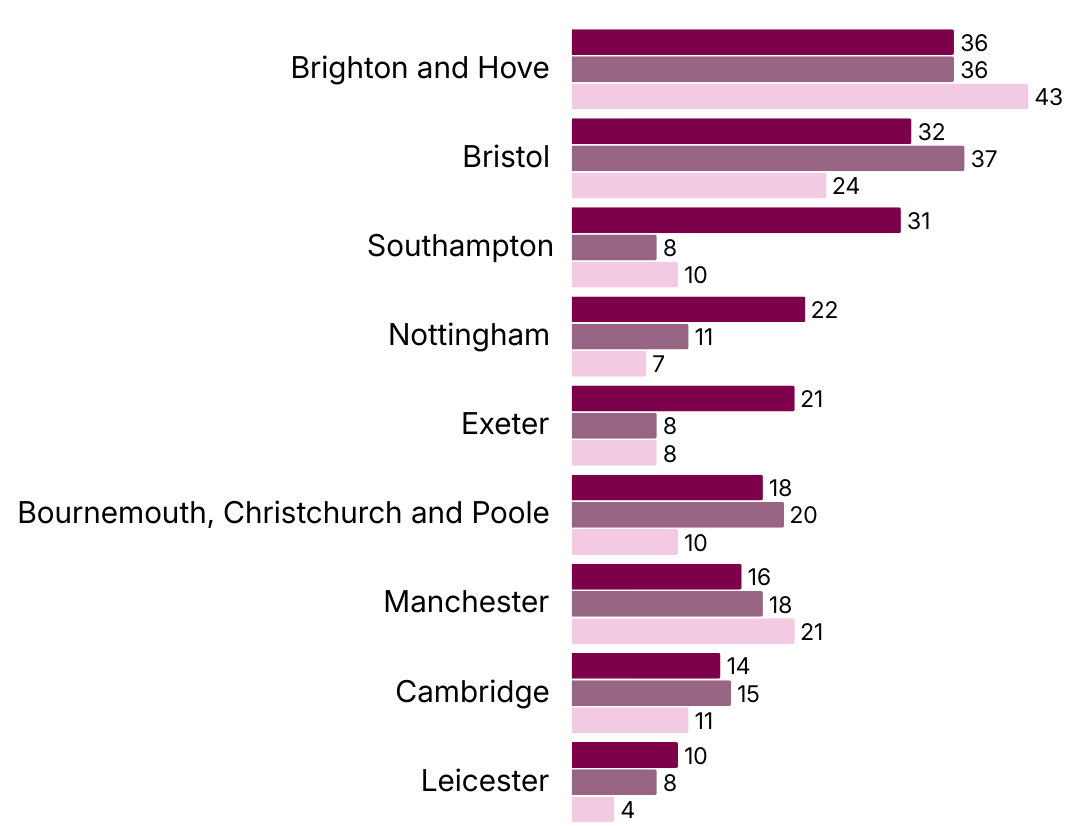
Number of reported deaths in England between 2022 and 2024 across selected Towns and Cities.
Research findings
This research focuses on investigations by Coroners into deaths of people experiencing homelessness. Where a Coroner identifies opportunities to save the lives of others, they have a duty to send a report to someone who can take action to save lives. Comparing all reports from Coroners in two periods: 2017-2021 & 2023-2025, the total number of reports sent has increased by around 46%.
However, comparing these two periods, reports in which the person who died was homeless have increased by over 250%, going from one or two a year in 2017 and 2018 to eighteen in 2025.
Furthermore, Coroners are now far more likely to identify that at a national level, they have specific concerns relating to housing and homelessness. It is for Coroners to decide who is in a position to take action to save future lives and so who they should write to. In the period 2017 2021, only 5 reports were sent to local/regional authorities with some responsibility for housing. In 2023-2025, 20 reports (a 567% increase) were sent to authorities with responsibility for housing, including seven sent to Central Government.
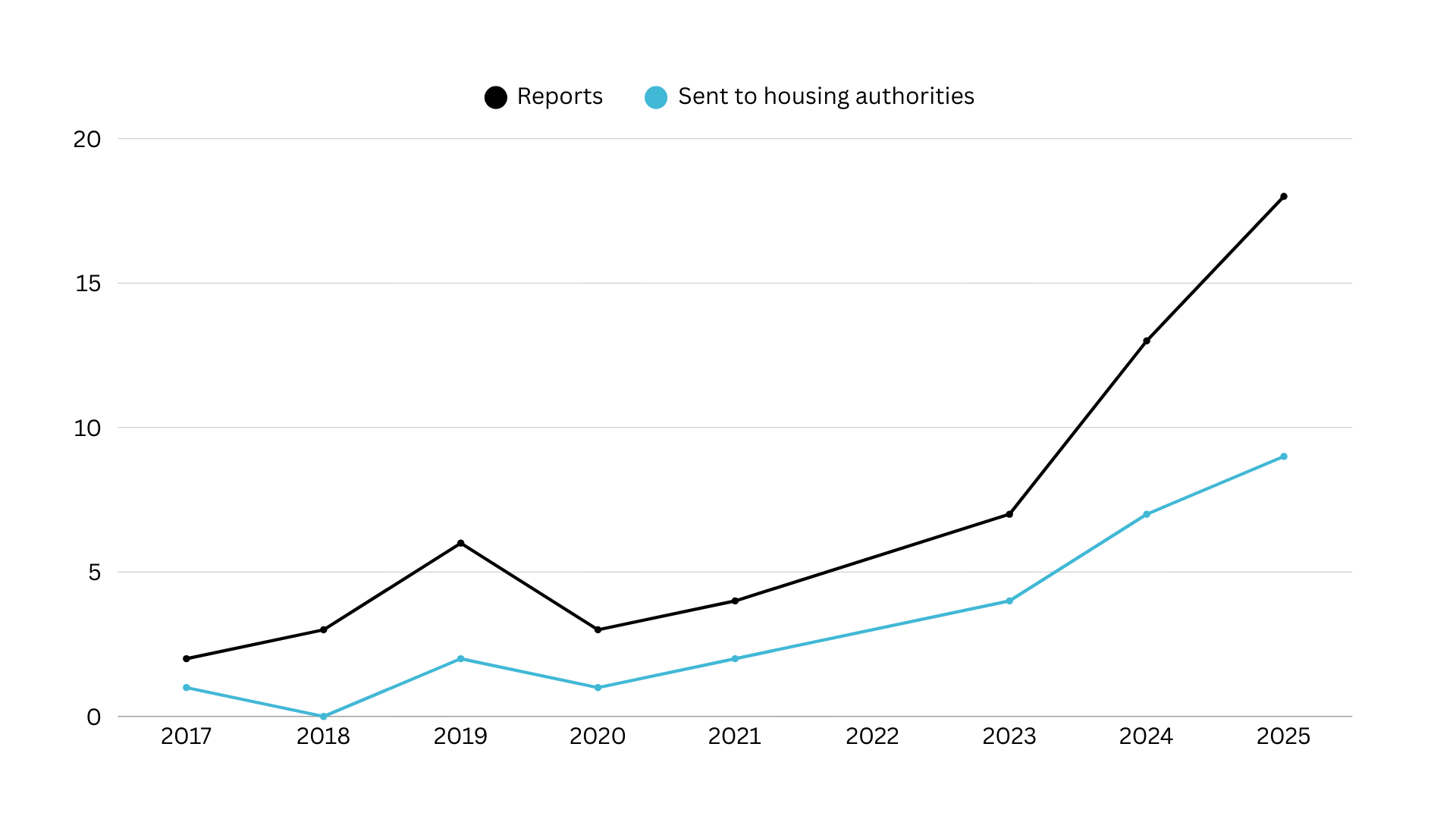
Coroner reports relating to the deaths of people experiencing homelessness (and numbers sent to housing authorities)
The research found that more reports treat housing/homelessness as central rather than peripheral, more engage with the need to prevent homelessness, and more set out issues which require substantive and system-level change.
However, there is a very wide variety in practice between different regions. In 2023-25, London accounts for one third of the reports, while a further 30% came from just 3 jurisdictions: Hull, Manchester South and Brighton. At the other end of the scale, in many other parts of the country in which people experiencing homelessness have died, no reports have been written, including cities like Bristol and Cambridge, and regions like the South East (excluding Brighton) and the East Midlands.
Recipients of a report must reply within 56 days. Some responses do little more than describe current law and policy without engaging with the Coroner’s concerns, while others identify action which is already being taken. A common weakness in responses is addressing only part of the concern expressed by Coroners or passing responsibility on elsewhere – for example, to suggest that the concern is about the specific administration of a policy by particular local authorities, rather than wider national concerns.
There is evidence that some Coroners are reviewing previous reports by other Coroners where they are investigating a similar case but this is not a consistent practice.
Case studies
Case study 1: the impact of the bedroom tax
Name: Lee McHale
Coroner: Alison Mutch, Senior Coroner for Manchester South
Report sent to: Ministry of Housing, Communities and Local Government
Concerns: ‘the property he resided in was larger than a single occupancy property because he had previously fostered children. As a consequence he was subject to the so called “bedroom tax”. This meant that there was a gap between housing benefit and his actual rent. Therefore he rapidly went into arrears with his rent and liable to be evicted. He did not feel able to deal with the situation. He was worried about moving from his home in part because he had allowed one of his now adult foster children to continue living with him. He had allowed that because he was concerned that person would otherwise become homeless.’
Response: The response from the Department for Work and Pensions does not propose any changes in response to the concerns raised by the Coroner. Their letter states that the policy is clear and additional support is available for claimants, but this is the responsibility of local authorities.
Case study 2: a systemic lack of care
Name: Joanita Nalubowa
Coroner: Harry Lambert, Assistant Coroner, Inner London
Report sent to: Ministry of Housing, Communities and Local Government
Concerns: Joanita Nalubowa was released from detention under the Mental Health Act 1983. Her family and support network were in London, and while she had been previously living in Teesside, she was divorced with few ties to the area, and concerns were raised that her ex-partner was abusive. Despite this, all London boroughs rejected her applications for accommodation in London, and the Coroner found that, the witness evidence was clear that there was no “discretion” and that London Boroughs and treating clinicians alike were powerless. The Deceased was therefore discharged to Stockton, against her wishes, against medical advice, away from her support network, and to an area where she would have to at best face her demons and at worst be in physical danger.
Shortly after being told she was being discharged to Stockton, the Deceased suspended herself using a ligature. ‘The evidence at the Inquest was that this situation is not uncommon, with those detained under the MHA not infrequently having social circumstances such that their historical place of residency is, for whatever reason, deeply inappropriate (or even dangerous).’ Response: The response from MHCLG notes that the ‘frameworks governing social housing and homelessness failed Ms Nalubowa in practice’ and the Secretary of State will write to local authorities to remind them of their statutory duties and their discretion to house vulnerable individuals (which they denied they had in this case). The focus of the response is on domestic abuse, including highlighting changes to rules which will exempt victims of domestic abuse from residency and local connections tests. However, the concerns expressed by the Coroner were broader than domestic abuse, and that is not acknowledged or explored in the response.
Policy recommendations
The Chief Coroner should:
- Ensure that published reports can be organised by reference to the wider determinants of health and inclusion health groups to enable them to more clearly connect to public health policy and practice and create a housing category. The database should also enable email alerts relating to specific areas.
- Ensure specific training for Coroners and officers on housing law, policy and practice, to explore trauma and deaths of despair drawing from the Dying Homeless project as well as family breakdown.
- Develop guidance supporting cross-referencing of reports.
Given clear evidence connecting homelessness and preventable deaths, all Coroners should ensure they comply with their statutory duty to identify risks of future deaths for people experiencing homelessness.
Central government must ensure they address the root causes of concerns raised by Coroners relating to homelessness. Proposals for a National Oversight Mechanism should be implemented to ensure lessons are learned from preventable deaths, including specific focus on homelessness. It should additionally consider means to enable the follow up and further scrutiny of issues identified in PFDs, and should work to ensure that training is provided for professionals involved in housing which sets out the issues identified in these PFDs, to seek to avoid similar circumstances arising in future.
The Ministry of Justice should include housing status in Coronial statistical returns
Further information
The individual reports are published by the Chief Coroner
Data from Dying Homeless 2025, Museum of Homelessness
Find out more about the project, including more detailed analysis of the reports identified: https://homelessinquests.blogs.bristol.ac.uk/
With thanks to the Museum of Homelessness. This work is dedicated to the memory of each individual who has died whilst experiencing homelessness.
The author
Dr Edward Kirton-Darling, Senior Lecturer University of Bristol Law School